by Guest Author | Apr 23, 2025 | Policy, Reports
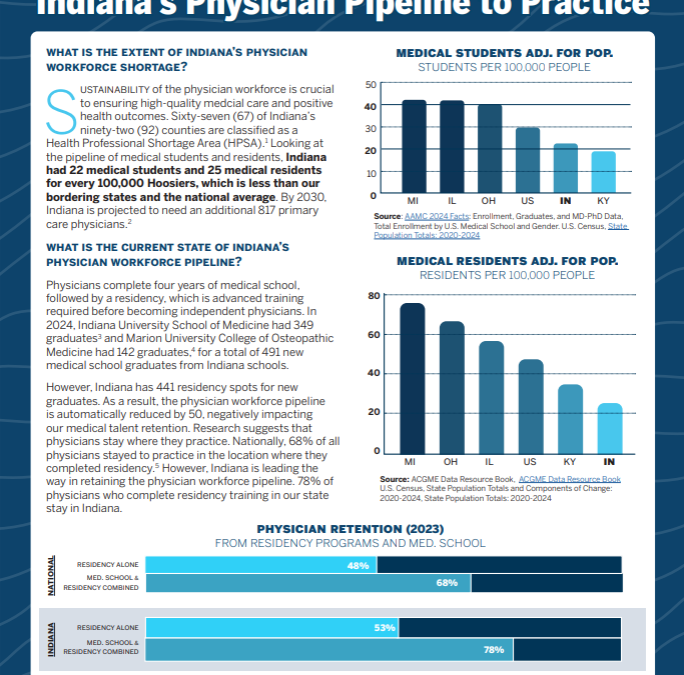
We released a brief report describing how Indiana’s physician pipeline-to-practice compares to our neighboring states and now comes the Bowen Snapshot: Indiana’s Physician Pipeline-to-Practice. This Snapshot summarizes the information included in the brief in just two pages! We hope this document succinctly communicates the state of Indiana’s physician pipeline and opportunities for strengthening it.
In addition to summarizing the extent of Indiana’s physician workforce shortage by looking at medical student and medical resident capacity, the Snapshot uses national data to quantify the size of the physician pipeline in 2024. It also describes the variation in state incentives to support the retention of doctors.
For more detailed insights, refer to the full snapshot below.
by Guest Author | Mar 13, 2025 | News, Policy, Reports
The Bowen Center’s newly released 2024 Annual Report showcases a year of significant achievements in health workforce research and policy. Highlights include completing the Playbook for Enhancing Indiana’s Mental and Behavioral Health Workforce, assessing Indiana’s EMS workforce, and finalizing a three-year direct care workforce project.
Under Dr. Hannah Maxey’s leadership, the Center has enhanced its data collection partnerships with state agencies while expanding its communication strategy to ensure research reaches decision-makers who need it most.
With a combination of funding from public and private sources, the Center produced 63 publications, delivered 22 presentations, and saw significant increases in website and social media engagement in 2024, solidifying its role as Indiana’s premier resource for health workforce planning.
The report also features testimonials from partners including Indiana Lt. Governor Suzanne Crouch and Indiana Professional Licensing Agency Executive Director Lindsay Hyer, who emphasize the Center’s crucial role in transforming workforce data into evidence-based solutions for healthcare access challenges across the state.
Download the full report here or read it in full below:
by Guest Author | Mar 13, 2025 | Policy
Indiana faces dental workforce shortages, with 68% of its counties designated as Dental Health Professional Shortage Areas (HPSAs). This shortage impacts access to essential oral health services for many residents. The Bowen Center for Health Workforce reviewed the current state of dental health professionals in Indiana, comparing it with neighboring states, and examines the potential of the Dentist and Dental Hygienist Compact to address these workforce shortages. Discover how interstate compacts could enhance mobility and reduce regulatory barriers for dental professionals.
Click here to read the full report and learn more about the dental health workforce in Indiana.
Read the full brief below or download it here.
by Guest Author | Feb 27, 2025 | Policy
You have seen our Indiana Medical Education Pipeline to Practice Report. Now you can take a deeper look into Indiana’s Physician Pipeline and how Indiana stacks up to our neighboring states with the Indiana Physician Pipeline-to-Practice: In Context brief. The medical education pipeline includes several steps before obtaining full medical licensure:
- Undergraduate Medical Education: Also known as medical school, this phase follows an undergraduate degree and lasts four years. It includes basic medical training and clinical hands-on experience with patients.
- Graduate Medical Education: This phase includes medical residency and fellowships. Residency is a structured series of clinical experiences preparing physicians to practice independently in their chosen specialty. Some physicians also complete additional fellowship training for 1-3 years.
- Practicing Physicians: These are fully licensed physicians who have completed all medical education requirements and can practice independently in their specialty.
The Bowen Center, along with the Indiana Department of Health, evaluated Indiana’s physician pipeline in family medicine, obstetrics/gynecology, and pediatrics. The study compares Indiana’s physician pipeline to neighboring states and national averages to support workforce planning.
Read and download the full brief below:
by Guest Author | Feb 26, 2025 | Policy
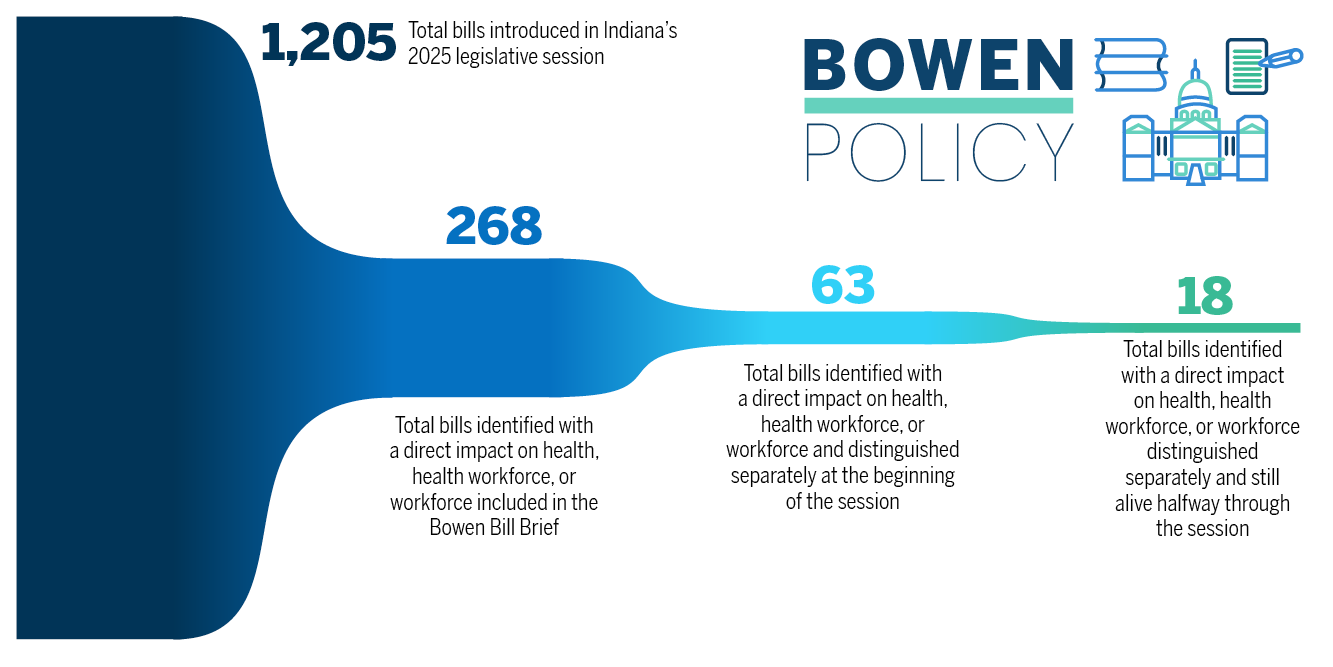
We are halfway through the legislative session. It has been a busy two months at the Statehouse. Introduced bills must have been heard in committee 3 times and then heard by legislators in the originating chamber by 2/20/2025. If a bill met these conditions and was approved by legislators, then it continued through the legislative process and will now undergo a similar process in the chamber that did not originate the bill. For a refresher on the legislative process, please see the Policy 101 page. As of 02/20/2025, of the almost 300 bills related to health, health workforce or workforce introduced this session, 63 are still considered active and are now working through the second chamber. The Bowen Center will continue to track these bills as the session continues. The 2025 legislative session ends on 04/29/2025. Continue reading below for a mid-session update.
See more information on our Bowen Bill Brief page.
Nursing Workforce
- SB 181 has entered the second chamber. This bill seeks to require trauma informed care training as part of the curriculum for a nursing education program.
- There is a shortage of Licensed Practical Nurses in Indiana. According to workforce projections by Health Resources and Services Administration (HRSA), Indiana currently has 72% of the licensed practical nurses (LPNs) necessary to support the needs of Hoosiers. SB 176 has moved to the House and seeks to remove barriers to becoming an LPN in Indiana. Check out our Bowen Center Snapshot to learn more about Indiana’s shortage of LPNs and how we compare to neighboring states.
- APRNs are licensed registered nurses (RN) with additional training that provides the clinical knowledge and experience to deliver advanced nursing care. Currently, all Indiana APRNs are required to hold an Indiana RN license, and many, but not all, also hold an APRN prescriptive authority license. The advanced practice registered nurse (APRN) workforce bills for this session didn’t make it out of committee hearings. SB 447 and HB 1151 would have established a license specifically for APRNs in Indiana. The Bowen Center compiled a report on APRN licensing strategies across the country, which you can review here.
Physician Workforce
- HB 1555 focuses on foreign trained physicians and has moved into the second chamber in the legislature. HB 1555 seeks to establish a limited medical license for those who have graduated from international medical programs, obtained a sponsor, and agreed to work in a medically underserved area. In 2021, 22% of actively practicing physicians licensed in Indiana reported completing their education in another country. Check out the education tab on the Bowen Center’s Indiana Physician Workforce Dashboard to get information on where Indiana physicians complete medical school and residency.
- SB 475 has entered the second chamber. SB 475 seeks to prohibit physician noncompete agreements.
- The two bills that focused on physician recruitment, HB 1068 and HB 1400 failed on first reading. HB 1068 sought to establish a program for medical school loan forgiveness while HB 1400 aimed to provide a tax credit for preceptors in medical education. Many other states have implemented tax credits to support recruitment and retention of clinical preceptors. The Bowen Center’s research on tax credits as an incentive strategy can be found here, including important considerations if Indiana were to implement something similar.
Behavioral Health
- Opportunities to streamline licensing while maintaining safety and quality were identified as a top priority by many stakeholders as part of the Playbook Project. HB 1520 and SB 216 include proposed changes to licensing policies for selected behavioral health professions. While HB 1520 did not pass out of the house, SB 216 is continuing through the second chamber.
- Workforce incentive bills HB 1154 and HB 1261 both did not pass out of the House. HB 1154 aimed to establish a behavioral health preceptor tax credit. This bill, hoping to support retention of clinical preceptors, would have provided a $1,000 state tax credit for a behavioral health professional who precepts a qualified student. HB 1261 sought to establish a behavior analyst license, which would have added a profession to the licensed behavioral health and human services workforce in Indiana.
Direct Care Workforce
- Currently, statute does not allow an individual with a felony offense related to substances to work as a CNA within five years of the offense. HB 1385 would alter this requirement to allow an exception if the CNA becomes certified as a peer recovery coach. HB 1385 has moved into the second chamber. You can review a summary of the Bowen Center’s 2024 research on direct care workforce data here.
- Two bills HB1161 and SB449 died in their respective originating chambers HB1161 sought to establish a license, training, and competency requirements for home health aides. SB 449 sough to require home health agencies to run a criminal background check on employees on an annual basis.
Other Health Workforce Matters
HB 1031 seeks to adopt the dentist and dental hygienist compact in Indiana. The dentist and dental hygienist compact would facilitate interstate practice of dentistry and dental hygienist in compact eligible states. If HB 1031 passes, Indiana will join ten other compact member states, and fifteen states with compact legislation pending.1 You can check out the 2022 Oral Health data here. Look out for the Bowen Centers 2024 Oral Health Reporting coming out later this year.
The Indiana pharmacy workforce plays a vital role in the provision of healthcare services to Hoosiers. SB 96 has moved to the House and would expand the immunizations that a pharmacist can administer to include those recommended and approved by federal agencies. Current law allows a pharmacist to administer immunizations approved by a physician. This bill would allow pharmacists to administer more immunization to Hoosiers who need them. The Bowen Center Pharmacist Workforce brief takes a deeper dive into services provided. Check out the latest Pharmacy Workforce Brief here.
Some additional bills that have moved into the second chamber but were not highlighted in our introduction blog post are outlined below.
| Bill Title |
Summary |
| HB 1200: Opioid Prescription Supply limits
|
This bill would establish limits for opioid prescribing to 180-day supply of certain drugs. |
| HB 1572: Hearing aids and speech language pathologists |
This bill would expand telehealth services to include speech-language pathologists. |
| SB 419: Crimes against health care providers |
Enhances protections for healthcare workers by increasing penalties for crimes committed |
| SB 473: Various health care matters |
Establish a separate registry for home health aides. Transfers administration authority to the nursing commission. |
All health workforce related bills remaining can be tracked using the Bowen Bill Brief. It has been an exciting first half of legislative session! The Bowen Center will continue to track all Health Workforce related bills until the end of session.
by Guest Author | Feb 18, 2025 | Data, Policy
Retention of medical students and residents is crucial to ensuring a strong physician workforce. This report examines retention within Indiana’s medical education pipeline between 2019 and 2024, challenges faced by residency program directors, trends in physician workforce capacity at Indiana hospitals, and existing initiatives supporting medical education and training in Indiana.
This work was completed in collaboration with the Indiana Department of Health. It is our hope that this report can inform discussions and policies targeting medical education in Indiana.
Read and download the project summary report below or find the full report here.