by Guest Author | Feb 13, 2025 | Policy
As of 2023, there were 9,134 Advanced Practice Registered Nurses (APRN) reported to be practicing in Indiana. These APRNs include Nurse Practitioners (NP), Clinical Nurse Specialists (CNS), Certified Nurse Midwives (CNM), and Certified Nurse Anesthetists (CRNA). APRNs are required to be licensed as Registered Nurses (RN) and meet certain educational criteria to provide APRN-level services. CNMs are the only APRNs required to hold a separate, dedicated license in Indiana. Many Indiana APRNs (NP, CNS, CNM only) hold a prescriptive authority license. This license enables APRNs to prescribe medications and requires collaborative practice agreements with a licensed physician, dentist, podiatrist, or optometrist. Approximately 71% of Indiana APRNs hold prescriptive authority licenses, meaning about 29% of RNs who self-identify as APRNs hold no APRN-level license.
In 2023, the Bowen Center conducted a fifty-state policy review of APRN licensing regulations and published the findings in a corresponding report. This policy review revealed that only Indiana and Wisconsin do not require APRN-level licensure for all practicing APRNs. Currently, Indiana has no formal process of tracking the number of APRNs, unless they are Certified Nurse Midwives, or hold prescriptive authority. Collection of data on APRNs is reliant on RNs self-reporting as APRNs. This leads to several potential challenges including the inability for individuals to easily verify credentials of APRN providers and lack of consistent and sufficiently granular data for workforce planning.
Based on the national policy review, the Bowen Center identified 4 prevailing implementation approaches to APRN licensure. SB447 and HB1151 aim to create separate licenses for each advanced nursing role, which aligns with Approach #4 outlined in the figure below.
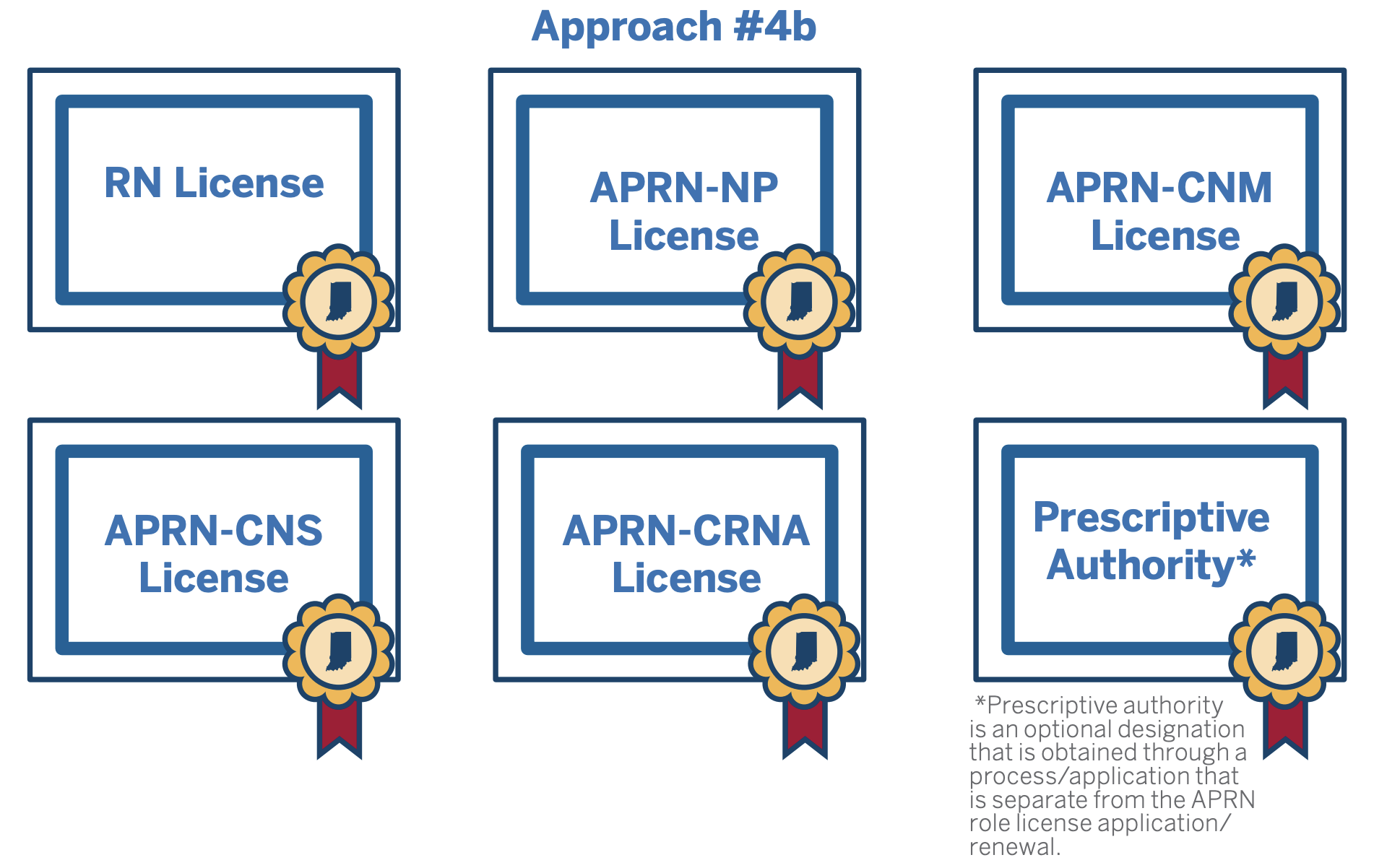
Regardless of the approach, it’s important that APRNs do not face a complicated licensure process. Key consideration include:
- Ensuring reciprocity and portability of licenses
- Reducing administrative burdens for license holders and state agencies
- Minimizing additional licensure costs
Professional regulation ensures quality service and public safety. The question to consider: Would an Indiana APRN license be helpful to protect public health and safety and support modernization of regulation, or are the current regulatory strategies sufficient?
Check out the full report here: Advanced Practice Registered Nurse Licensing.
by Guest Author | Feb 10, 2025 | Playbook, Policy
In 2023, a significant number of Indiana’s youth faced severe mental health challenges. Nearly half of high school students reported experiencing depression, and a quarter of them had gone as far as developing a plan for suicide. This highlights the urgent need for mental health support and intervention among young people in the state.
Issues with access to care are widespread. In 2024, more than 65% of Indiana adolescents with depression were unable to access care. All of Indiana’s 92 counties contain a federally designated mental health workforce shortage. Without sufficient capacity to address concerning mental health issues, children and youth run the risk of falling through the cracks. Schools are uniquely positioned to support overall student well-being because they serve as a consistent point of access within their communities. Indiana law requires schools provide several services intended to support the mental, emotional, and behavioral health and wellness of students including student assistance services.
These services are required to be provided by professionals licensed by the Indiana Department of Education (DOE), including school counselors, school social workers, and school psychologists. While schools are authorized in statute to support students’ emotional and behavioral health, anecdotal reports indicate difficulties with school-based behavioral health workforce capacity.
Currently, state level data is limited and does not include information related to services. More information is needed to support and elevate these integral workers. Recognizing this gap in necessary information, the DOE, with support from Indiana Department of Health, administered a pulse check survey to school counselors, social workers, and psychologists. Findings from this pulse check are included here, as well as recommendations for next steps.
Download the full PDF of the report here or check out the interactive version below (PDF also follows the interactive version below).
See the full report with our findings in the PDF below:
by Guest Author | Jan 29, 2025 | Policy
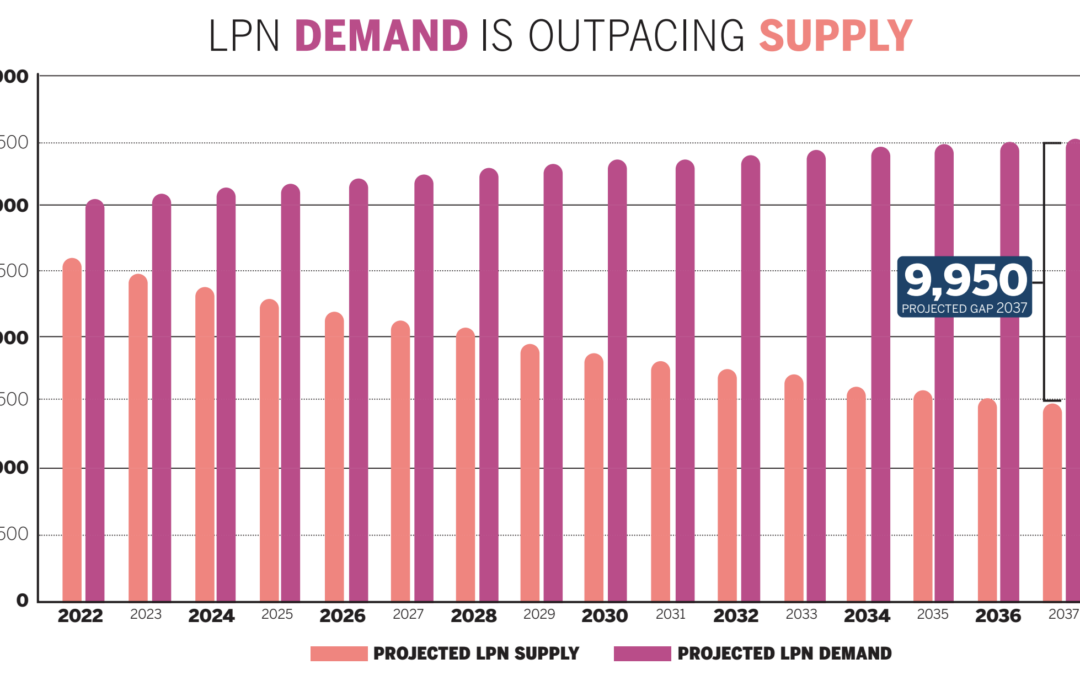
The Bowen Center recently analyzed state and national trends to examine whether Indiana faces a shortage of Licensed Practical Nurses now and into the future.
Check out the findings below:
You can also read or download the above in PDF form here:
by Guest Author | Jan 29, 2025 | Policy
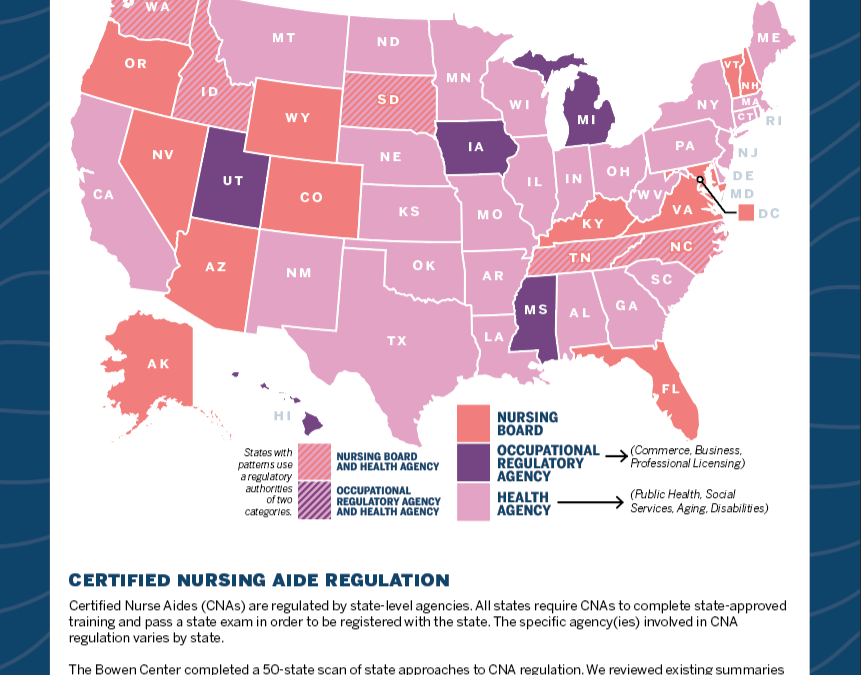
Certified Nursing Aide Regulation
Certified Nurse Aides (CNAs) are regulated by state-level agencies. All states require CNAs to complete state-approved training and pass a state exam in order to be registered with the state. The specific agency(ies) involved in CNA regulation varies by state.
The Bowen Center completed a 50-state scan of state approaches to CNA regulation. We reviewed existing summaries from 2022 and 2024, and explored current statutes and administrative codes to categorize state approaches to regulation as being led by the nursing board, occupational regulatory agency, health agency, or a combination. The map below shows the results of the scan.
Read or download the above blog post in PDF form here:
by Guest Author | Jan 28, 2025 | Data, Policy
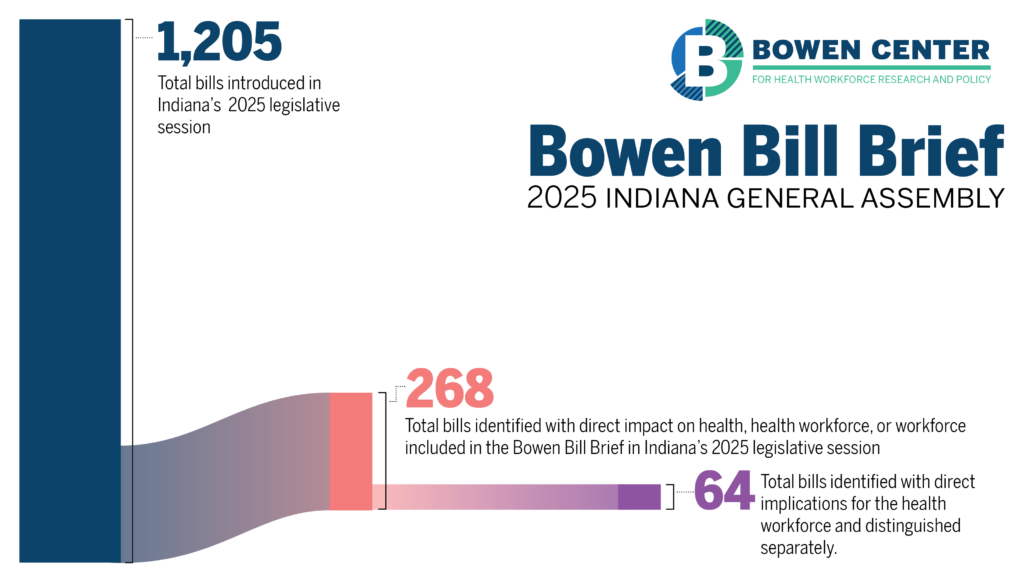
The 2025 legislative session is in full swing, and the landscape just got easier to navigate. Almost 300 bills related to health, the health workforce, or the workforce generally were introduced this session. The Bowen Center will be tracking these bills as the session continues. While you’ll still find our comprehensive bill tracking table with all the details on each bill being considered, we’re excited to introduce a new dynamic dashboard that puts the session’s pulse at your fingertips. Our interactive infographic gives you real-time insights into the status of health care workforce legislation, from start to finish, across both chambers. Whether you’re tracking workforce initiatives, regulatory changes, or public health measures, you can now visualize the flow of bills through the legislative process and quickly identify trends in health care policy priorities. We have summarized a few pieces of legislation below that intersect with work previously done by the Bowen Center. Check out the dedicated Bowen Bill Brief page for full details on all the bills we’re tracking.
Nursing Workforce
- There are several bills this session focused on the advanced practice registered nurse (APRN) workforce. SB 447 aims to establish a license specifically for APRNs in Indiana. APRNs are licensed registered nurses (RN) with additional training that provides the clinical knowledge and experience to deliver advanced nursing care. Currently, all Indiana APRNs are required to hold an Indiana RN license, and many, but not all, also hold an APRN prescriptive authority license. In 2023, the Bowen Center completed a national review of state approaches to APRN licensing to see how Indiana’s approach compared to other states. Only one other state (Wisconsin) has an approach similar to Indiana’s, and this is still the case in 2025. Check out the full report here.)
Physician Workforce
- Indiana is facing a physician workforce shortage due to multiple factors, including burnout, an aging population, and competition from other states. Both HB1068 and HB1400 focus on workforce incentives targeted toward retaining physician talent in Indiana. HB1068 seeks to establish a program for medical school loan forgiveness while HB1400 seeks to provide a tax credit for preceptors in medical education. Many states have used tax credits to retain and recruit the clinical preceptors required for health professions’ education. In 2024, the Bowen Center reviewed tax credits as an incentive strategy for clinical preceptors using data from other state program evaluations. More information can be found here, including considerations for Indiana.
- Recruitment of physicians plays a role in alleviating physician workforce shortages. HB 1555 focuses on the recruitment of foreign trained physicians to Indiana. HB1555 seeks to establish a limited medical license for those who have graduated from international medical programs, obtained a sponsor, and agreed to work in a medically underserved area. In 2021, 22% of actively practicing physicians licensed in Indiana reported completing their education in another country. This suggests that HB1555 may have significant impacts on workforce supply. Check out the education tab on the Bowen Center’s Indiana Physician Workforce Dashboard to get information on Indiana Physicians who completed medical school in another country.
Behavioral Health
- All of Indiana’s 92 counties contain a federally designated mental health workforce shortage. As a part of the Playbook Project, the Bowen Center convened stakeholders to discuss challenges and opportunities for strengthening the pathway to practice for the mental and behavioral health professionals in Indiana. Opportunities to streamlining licensing while maintaining safety and quality were identified as a top priority by many stakeholders. HB1520 and SB216 include proposed changes to licensing policies for selected professions.
- Workforce incentives were another priority identified by stakeholders during the Playbook Project. Incentives are needed to recruit and retain qualified behavioral health and human services professionals into the workforce. HB1154 aims to establish a behavioral health preceptor tax credit. This bill, in hopes of aiding retention, would provide a $1,000 state tax credit for a behavioral health professional who precepts a qualified student. HB 1261HB 1261 seeks to establish a behavior analyst license, which would add a profession to the licensed behavioral health and human services workforce in Indiana.
Direct Care Workforce
- Indiana’s population is steadily getting older, with an estimated 1 in 5 Hoosiers over the age of 65. An aging population typically indicates a greater demand for health care professionals, specifically direct care workers, such as home health aides (HHAs) and certified nursing aides (CNAs). HB1161 would establish a license, training, and competency requirements for home health aides. SB 449 would require home health agencies to run a criminal background check on employees on an annual basis.
- Currently, statute does not allow an individual with a felony offense related to substances to work as a CNA within five years of the offense. HB1385 alters this requirement to allow an exception if the CNA becomes certified as a peer recovery coach. The Bowen Center is excited to launch workforce dashboards for CNAs, HHAs, and qualified medication aides later in 2025! In the meantime, you can review a summary of research we completed in 2024 on direct care workforce data here.

by Guest Author | Jan 15, 2025 | News, Policy
Indiana’s Health Workforce Council is exploring an approach to strengthen rural health care training: a tax credit for health care providers who mentor students through clinical preceptorships. Bowen Center Director Dr. Hannah Maxey was recently quoted in IPB News discussing the possible tax credit program for health care mentors.
“It is critically important for states that are developing tax credit programs to clearly define the program, goals and metrics before and prior to developing it,” Maxey notes. Her research indicates these programs typically serve better as retention tools for existing clinical preceptors rather than recruiting new ones.
Want to learn more about Maxey’s insights on program design, retention impacts, and fiscal considerations? Read the full story at IPB News.
The Bowen Center recently published a policy brief on exactly this subject, read more here or in the brief below: